Surgical techniqueThe aim of the surgical procedure is to close the fistula in layers and to strengthen the posterior tracheal party wall. If the stoma needs revision, this can be accomplished at the same time (see the following chapter on stoma revision).
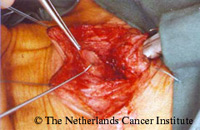
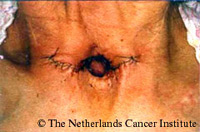
The figure to the right is showing a case of a hypertrophic, too low situated fistula, which caused persistent leakage around the prosthesis. An incision is made horizontally on either side of the stoma, and curved posterior to encompass the posterior line of the stoma and a superiorly based skin and platysma flap is created (see figure below to the right right). |
 |
|
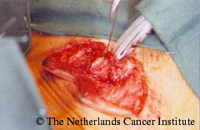
The figure to the right shows the posterior tracheal wall is dissected away from the esophagus, revealing the fistula tract (figure below to the right).
|
  |
|
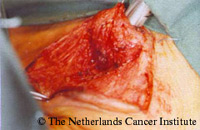
The TE-fistula is then completely dissected free to enable a hemostat being passed underneath (figure to the right). The fistula is opened and cut completely (figure below to the right).
|
  |
|
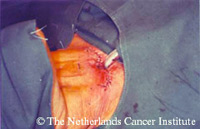
The esophageal stump is closed with inverting vicryl sutures (figure to the right). A second muscular layer is sutured to reinforce the esophageal wall. If needed, the sternal head of the sternocleidomastoid muscle can be dissected from the sternum to create a superiorly based muscle flap, which can be easily interposed between the esophagus and the trachea. Even if this additional layer is not needed, it is advisable to take this opportunity to cut the sternal heads of the sternocleidomastoid muscles. This has the advantage that the stoma area will be flatter after this procedure, which makes the use of stoma appliances, such as an HME or automatic stoma valve, easier, as already described earlier in the chapters on total laryngectomy and tracheostoma construction.
|
 |
|
Next the tracheal wall is sutured in one layer (figures to the right).
|
  |
|
Finally, the skin is closed in one layer (figure to the right). No wound drains or dressings are required generally. The figure below to the right is showing the final situation at the end of the procedure. A secondary tracheal puncture can be carried out after complete healing of the stoma, mostly after 6 weeks.
|
  |