Surgical technique of secondary TE puncture and introduction of the Provox voice prosthesis
The instruments needed for this procedure are besides the contents of the original Provox (1) package, i.e. the voice prosthesis (of a proper length), the guide wire and the scalpel, or in case the Provox2 device is used, a prosthesis with the proper length and a separately packed guide wire, a short rigid esophagoscope with a light source, the Provox trocar and cannula and 2 curved non-toothed hemostats (figure above). The secondary puncture is performed under peri-operative 24 hours broad-spectrum antibiotic prophylaxis.
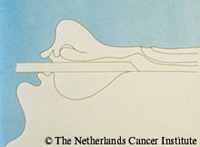
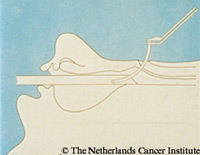
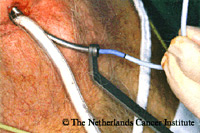
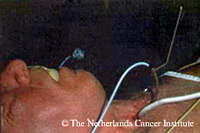
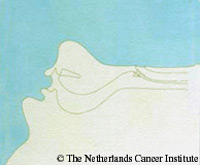
The laryngectomized patient is intubated. The short rigid esophagoscope is introduced and moved towards the tracheostoma (figures right). In case of a stenosis, it might be helpful to introduce a thin nasogastric tube first, to facilitate the introduction of the scope and to guide the dilatation, which should be carried out first. When the tip of the esophagoscope reaches the tracheostoma, the scope is swiveled 180o, turning the oblique open side of the esophagoscope upwards. An assistant keeps the instrument in this position. By removal of the ventilation tube of the anesthetist, a clear view inside the tracheostoma is obtained. The proper position of the scope is checked by palpation with a finger. At this stage, selection of the proper size of the prosthesis should be made. The thickness of the tracheoesophageal party wall is also judged with the palpating finger. Four lengths of the Provox voice prostheses are available: 4.5, 6, 8 and 10 millimeters, and two additional lengths of 12.5 and 15 mm of Provox2. In most patients an 8 or 10 millimeter prosthesis is sufficient. In case of doubt, use the longer prosthesis to allow for postoperative swelling and edema at the puncture site. The trocar and cannula is then placed in the midline of the tracheoesophageal wall, 5 mm below the mucocutaneous junction, and a TE fistula is created by puncturing towards the lumen of the scope. The sharp tip of the trocar is caught in the esophagoscope under visual guidance of the assistant (figures right). The cannula is removed and the flexible guidewire introduced through the trocar. The connector appears in the esophagoscope and is pushed upwards (figures). The esophagoscope is now removed and the Provox voice prosthesis is attached to the connector head of the guide wire (figures below). By pulling the guide wire inwards, the introduction string of the prosthesis is introduced into the TE fistula. During this procedure the ventilation tube of the anesthetist is re-introduced for a few minutes. Finally after removal of the ventilation tube again, the prosthesis is pulled and rotated into the TE fistula with the help of two curved non-toothed hemostats (figures). The introduction string is cut. The prosthesis is then turned in its proper position with the oval side of the flange pointing downwards in the trachea (figures). After the patient is awake, the impermeability for liquids of the prosthesis and the TE fistula is checked by drinking of water. If there is no leakage, an oral feeding can be resumed right away. Speech therapy usually also starts the same day. Reminder: It is important to place the Provox voice prosthesis at the correct position in the tracheal back-wall, i.e. the puncture should be carried out in the midline 5 mm below the upper tracheal rim, causing the upper border of the tracheal flange of the prosthesis almost to reach the mucocutaneous junction. A too low position of the prosthesis leads more easily to leakage, makes cleaning and replacement more difficult, and might result in less optimal speech. |
             |