Surgical technique of primary TE puncture and introduction of the Provox voice prosthesis
At this stage of the surgical procedure the primary tracheoesophageal puncture (TE) is carried out. No temporary stenting of the TE-fistula is needed with the Provox system. First, the proper size of the voice prosthesis should be selected. For this reason, the thickness of the tracheoesophageal party wall should be judged with a palpating finger. The original Provox prosthesis is available in four lengths: 4.5, 6, 8, and 10, millimeters, and the Provox2 device in two additional lengths, 12.5 and 15 mm. In most patients an 8 or 10-millimeter prosthesis is appropriate. In case of doubt, use the longer prosthesis to allow for postoperative swelling and edema at the puncture site.
The use of the special Provox pharynx protector is recommended. This instrument can be placed through the open pharynx into the cervical esophagus and positioned just cranially of the tracheostoma. The use of the Provox trocar and cannula is recommended for the TE-puncture (figure right). If this instrument is not available, a non-cutting sharp trocar is preferred over any cutting device, e.g. a scalpel, because this could cause an oval shaped TE fistula tract. The trocar is placed in the midline of the trachea back wall 5 mm under the upper tracheal mucosa rim. The trocar is directed towards the opening of the pharynx protector. With a slight twisting movement of the hand, a clean hole is punctured in the tracheoesophageal party wall. |
  Closure of the pharynx is carried out in a T-shape. This enables a low-tension closure, tailored to the size of the defect and avoids the development of a ridge at the base of tongue i.e. the formation of a “neo-epiglottis”. Before closure of the pharynx is carried out, a nasogastric feeding tube is brought into position. The mucosa is closed with running atraumatic vicryl 3-0 sutures with a round needle starting cranially and laterally (figure below). Tissue surplus caudally is closed with a purse string suture.
A second submucosa layer is also closed with running sutures. Finally the pharyngeal constrictor muscle is closed, running or with mattress sutures. This layer should not be closed too tightly. The figure to the right is showing the PE segment after closure of the muscle layer. 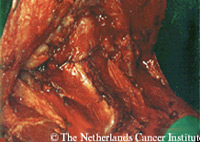 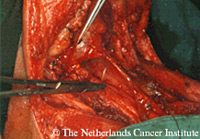 |