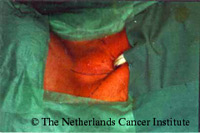
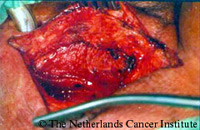
Surgical constrictor pharyngeus myotomyThe surgical technique is as follows: a vertical paramedian skin incision is made on the side of the hemithyroidectomy and or neck dissection (figure). Care is taken not to damage the carotid artery, which in most patients is displaced medially. The pharynx is dissected free carefully (figure right). If nerve branches of the plexus pharyngeus are seen, they should be severed. A meticulous paramedian myotomy is then performed, cutting the last muscle fiber, without entering the pharyngeal lumen.
This is greatly facilitated by the introduction of a cuffed anesthesia tube into the pharynx, prior to the surgical procedure. By inflating the balloon of this tube and moving the tube slightly up and down, it can be easily seen whether the last muscle fibers have been cut. The figure below to the right is showing the inflated balloon after the complete myotomy and the figure to the right the situation with the deflated balloon. The full length of the constrictor pharyngeus muscle should be myotomized. Especially high up at the base of tongue no muscle fibers should be forgotten. The wound is closed in layers, after leaving a small diameter suction drain behind. The result of this procedure can be judged usually already on the first postoperative day. |
    |