Provox2 voice prosthesisReplacement of the Provox2 voice prosthesis is carried out with a disposable insertion tool (a loading tube and an inserter) for the anterograde insertion of the voice prosthesis directly through the stoma into the TE-fistula. This 'second generation' device has been adapted for anterograde insertion by having softer flanges (the esophageal flange being the more rigid one), and more curved junctions between the flanges and the shaft. This allows easier insertion in the loading tube and facilitates removal out of the TE fisula tract with a hemostat. The diameter of the shaft has not been changed, but the thickness of the esophageal flange is decreased from 1.6 mm to 1.5 mm, and of the tracheal flange from 1.6 mm to 1.3 mm. The size (=distance between the flanges) of the prosthesis is marked on the tracheal flange, to facilitae identification of the length of the prosthesis in situ. Sizes are 4.5, 6, 8, 10, 12.5 and 15 mm.
Loading of the Provox2 voice prosthesis into the insertion tool: the insertion tool consists of an inserter and a loading tube. The inserter has 2 mark-lines: number 1 is the line indicating the correct position of the prosthesis in the loading tube; number 2 is the line indicating that the esophageal flange is unfolded just outside the tip of the loading tube. The safety string of the voice prosthesis is inserted into a slit of the inserter, and pulled in place to secure its position. Thereafter, the prosthesis is placed on top of the inserter (figure 1).
Next, the esophageal flange of the voice prosthesis is squeezed between thumb and index finger and hooked into the loading tube ensuring that the esophageal flange is folded forward (figure 2). The thumb of the other hand should push down and forward the flange, which is still protruding from the slit of the loading tube (figure 3). This flange has to be kept down firmly within the tube, while pushing the inserter forward until mark-line 1 is reached. Now the prosthesis is in the correct position for insertion (figure 4).
To prevent accidental loss during its insertion, the Provox2 prosthesis has a security string, which extends in the axis of the flange and can also serve as the introduction string, if the voice prosthesis is inserted in the traditional retrograde manner through the pharynx. The possibility to replace this prosthesis both in an anterograde and in a retrograde manner makes the Provox2 prosthesis the most versatile prosthetic device presently available. The anterograde replacement procedure appears to be easily accomplished not only by Otolaryngologists, but also by other medical professionals, such as speech pathologists and oncology nurses (see videoclip). Local anthesia is seldom necessary. In some patients, the procedure may cause slight coughing reflexes, which might be dampened with a 4 och 10% lidocain spray into the trachea. Local anesthesia in the pharynx is not needed. |
 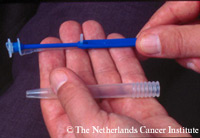 Figure 1.
 Figure 2.
 Figure 3.
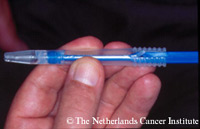 Figure 4.
|
|
Replacement of the Provox2 prosthesis: the old Provox2 prosthesis is removed from the TE-fistula by pulling out the device with a non-toothed hemostat (see video at the end of this chapter). (In case a 'Provox1' prosthesis has to be removed, the Provox guide wire may be used for retrograde transoral removal, as described below).
Alternatively, up to the clinician's discretion, the tracheal flange might be grasped with a hemostat and cut off, and the remainder of the device is pushed into the esophagus, allowing for natural passage through the intestinal tract. The patient's clinical history of abdominal diseases should hereby be taken into account. The loading tube is inserted into the TE-fistula (figure 5) until the back wall of the esophagus is slightly touched. Then, with the loading tube kept in this position with one hand, the inserter, grasped between thumb and index finger of the other hand, is pushed forward until mark-line 2 is reached. The thumb should be used as an additional stopper, to keep the tracheal flange inside the loading tube at this time. In this position the forward folded esophageal flange is unfolded in the lumen of the esophagus. Next, the complete insertion tool, this is the loading tube and the inserter toghether, is pulled back, anchoring the esophageal flange on the anterior esophageal wall. Then, the loading tube can be slid backwards, keeping the inserter in place, allowing the tracheal flange of the voice prosthesis to unfold properly (figure 6). Sometimes, this happens immediately. In other cases, the tracheal flange has to be unfolded deliberately, either by turning the inserter with the prosthesis around its axis, or by turning and pulling this flange into position with a non-toothed hemostat. The proper position of the voice prosthesis can be checked easily by rotating and exerting slight traction on the tracheal flange, after which the safety string of the prosthesis can be cut off with a small pair of scissors, or a scalpel (figure 7). The Provox2 voice prosthesis is then ready for use. |
 Figure 5.
 Figure 6.
 Figure 7.
|
Provox2 replacement video clip: loading insertion device
Provox2 replacement video clip: removal of old prosthesis
Provox2 replacement video clip: immediate insertion and overshooting examples