Replacement of the Provox (1) voice prosthesis
Video clip is animation of the replacement procedure.
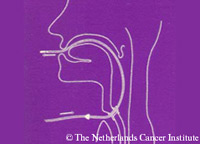
1) Obtain satisfactory local anesthesia of the trachea and oropharynx with lidocain 10% spray. Some experienced patients might prefer replacement of the prosthesis without local anesthesia, since the lidocain spray causes the same or sometimes even more irritation than the rapid replacement procedure itself. Introduce the guidewire through the old prosthesis and push it upward through the pharynx and out of the mouth. Often it is easy to grab the guidewire in the pharynx with a finger. Sometimes the introduction of the guidewire needs special attention. This is particularly true for the low positioned prosthesis. Grasping the tracheal flange with a non-toothed hemostat and changing the position of the prosthesis in a more upright direction, can facilitate the proper movement of the wire into the pharynx. In the rare event that the wire is trapped at the base of the tongue or tonsil, a tongue depressor and hemostat are useful in freeing the guidewire.

2) Grasp the tracheal flange of the prosthesis with a curved non-toothed hemostat, cut this off from the prosthesis with the disposable scalpel, included in the package, and remove it over the guidewire
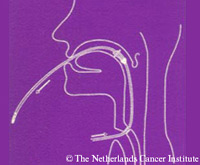
3) Remove the esophageal remnant of the prosthesis transorally with a push and pull action of the disposable guide wire that has a 8 mm stop halfway its length for this purpose.
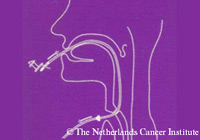
4) Attach the new Provox voice prosthesis to the connector of the guidewire and secure it in its slid with a gentle pull of the introduction string of the prosthesis. Pull the wire the prosthesis towards the existing TE-fistula and ask the patient to swallow the new prosthesis.
5) Introduce the prosthesis into the TE-fistula. Because of the oval shape and flexibility of the tracheal flange the prosthesis can be introduced easily into the fistula, mostly with the help of the curved non-toothed hemostat. Finally, the introduction string is cut off with the disposable scalpel.
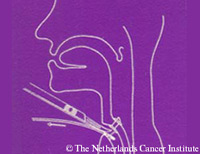
6) The prosthesis in situ after removal of the introduction string, ready for speech. Preferably, the long end of the tracheal flange points downward in the trachea