Leakage around the prosthesis even with the shortest length (4.5 mm)Problem: the patient has leakage around the prosthesis and the shortest (4.5 mm) prosthesis is already in situ. Atrophy of the tracheoesophageal party wall is a problem that is encountered with all the presently available voice prosthesis systems. This is a real fistula, i.e. tissue-related and not a device-related problem. Most probably, this atrophy is mainly a side effect of radiotherapy.
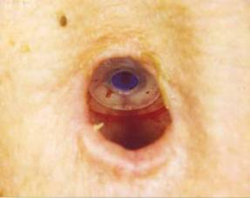
Immediately after replacement, a slight leakage around the prosthesis may occur for some hours or a few days, but this may well be decreasing spontaneously. Therefore, a short observation time is advisable. However, if this leakage does not decrease spontaneously, there are several solutions for this atrophy problem. First of all the formation of an esophageal pouch (overgrowth of mucosa over the posterior flange) can mimic this atrophy and in these cases there is no real atrophy, and a shorter prosthesis is not indicated. In stead a longer prosthesis should be inserted. The traditional option is temporary (often several days) removal of the prosthesis and insertion of a cuffed trachea cannula and/or nasogastric feeding tube to allow for shrinkage of the fistula. Obviously, this is uncomfortable for the patient, and may require hospitalization of the patient. Therefore, we prefer an instant and for the patient more comfortable solution, which is initially to put a thin (0.5 mm) silicon ring (Provox XtraFlange) behind the tracheal flange: see picture (see movie). If leakage around persists or recurs, the application of a purse string suture around the fistula tract, using an atraumatic absorbable 3.0 vicryl suture can be used. The procedure is shown schematically in upper figure. First the old prosthesis is removed and the suture is inserted submucosally at 12 o’clock at a distance of 1-2 mm of the fistula edge (top-left). The needle is curved around the fistula tract, coming out at 6 o’clock. The needle is inserted again and curved upward submucosally to 12 o’clock again (top-right). Then, the new prosthesis is inserted and the suture is carefully tied, causing the fistula wall to be tightened around the prosthesis (bottom left and right). The middle and lower figure show a typical case pre and post suture placement. The suture should not be removed, but left for spontaneous absorption.This has an augmentation effect on the fistula wall, curing the problem. A short course of a broad-spectrum antibiotic treatment should be given to prevent local infection. If leakage around the prosthesis is intractable to more conservative surgical measures, surgical closure of the fistula and subsequent re-puncture may be necessary (see chapter Surgical procedures). |
    |