Leakage around the prosthesis and the prosthesis is too long
Issue: the patient experiences leakage around the prosthesis and the prosthesis is too long.
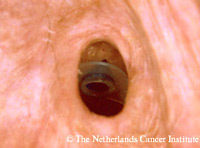
After primary or secondary TEP, subsiding of the inevitable surgical edema and tissue reaction is a natural course of events, especially with indwelling voice prostheses, which are not handled by the patients themselves (little trauma to the fistula). This means that during follow-up gradually the prosthesis might become too long (see figure right). If in the mean time no replacement for leakage through the prosthesis was necessary, this might result in a ’pistoning’ of the prosthesis during swallowing, whereby fluids are squeezed around the prosthesis, leading to aspiration and coughing (see figure and animation right ). This problem often can be solved easily by inserting a shorter prosthesis or a silicon ring around the shaft posterior to the tracheal flange. From our experience it is probably better not to downsize more than one size, because a too tight fit might cause swelling and edema, making the device quickly too short, whereas a slightly too long device is much less problematic. One should be careful not to interpret all prosthesis protruding a little in the trachea with leakage around as too long prostheses. Formation of an esophageal pouch (overgrowing of esophageal mucosa over the the posterior flange) can simulate a too short prosthesis whereas in fact a longer prosthesis is needed in these cases.
After primary or secondary TEP, subsiding of the inevitable surgical edema and tissue reaction is a natural course of events, especially with indwelling voice prostheses, which are not handled by the patients themselves (little trauma to the fistula). This means that during follow-up gradually the prosthesis might become too long (see figure right). If in the mean time no replacement for leakage through the prosthesis was necessary, this might result in a ’pistoning’ of the prosthesis during swallowing, whereby fluids are squeezed around the prosthesis, leading to aspiration and coughing (see figure and animation right ). This problem often can be solved easily by inserting a shorter prosthesis or a silicon ring around the shaft posterior to the tracheal flange. From our experience it is probably better not to downsize more than one size, because a too tight fit might cause swelling and edema, making the device quickly too short, whereas a slightly too long device is much less problematic. One should be careful not to interpret all prosthesis protruding a little in the trachea with leakage around as too long prostheses. Formation of an esophageal pouch (overgrowing of esophageal mucosa over the the posterior flange) can simulate a too short prosthesis whereas in fact a longer prosthesis is needed in these cases.